
Abstract
India's public health insurance architecture anchored by PM-JAY covers over 500 million citizens, yet remains heavily weighted toward late stage tertiary care. The result is a system where the financial burden of treating advanced cancers, complex cardiovascular disease, and late presenting rare conditions consumes a disproportionate share of public health expenditure. This blog explores a pivotal question can mass healthcare schemes like PM-JAY economically support early biomarker detection and AI driven molecular screening? Health economics increasingly says yes and the calculus becomes even more compelling when precision diagnostics are deployed at scale through platforms like Genix.ai.
Can Mass Public Healthcare Schemes Like PM JAY Afford Precision Diagnostics?
Yes and the economic argument is stronger than most policymakers currently acknowledge.
PM-JAY (Pradhan Mantri Jan Arogya Yojana), the insurance arm of Ayushman Bharat, is one of the world's largest government funded health protection schemes. It covers hospitalisation costs for over 100 million vulnerable families across India. However, the majority of PM-JAY claims are driven by late stage conditions advanced cancer, end stage renal disease, cardiac surgeries where the cost per episode is high, outcomes are uncertain, and recurrence tracking adds compounding expenditure over years.
The core problem is not the scheme itself. It is where the clinical intervention happens on the disease timeline.
When a patient enters the healthcare system at Stage III or Stage IV cancer, the care pathway becomes immediately expensive: chemotherapy cycles, radiation, ICU admissions, surgical interventions, palliative management, and regular imaging follow ups. The five year survival rates at these stages remain low particularly for cervical, oral, and colorectal cancers, which are among the most common in India's lower income populations.
Contrast this with Stage 0 or Stage I detection. At these stages, surgical excision or targeted molecular therapy is often curative, the treatment pathway is shorter, and long term recurrence monitoring costs are substantially lower. The financial case for early detection is not speculative it is built on decades of oncology health economics research.
Integrating early biomarker screening and genomic risk profiling into PM-JAY's preventive health tier is not a luxury upgrade to the scheme. It is a structural cost reduction strategy.
Re balancing the Cost Curve: Late Stage Therapy vs. Molecular Screening
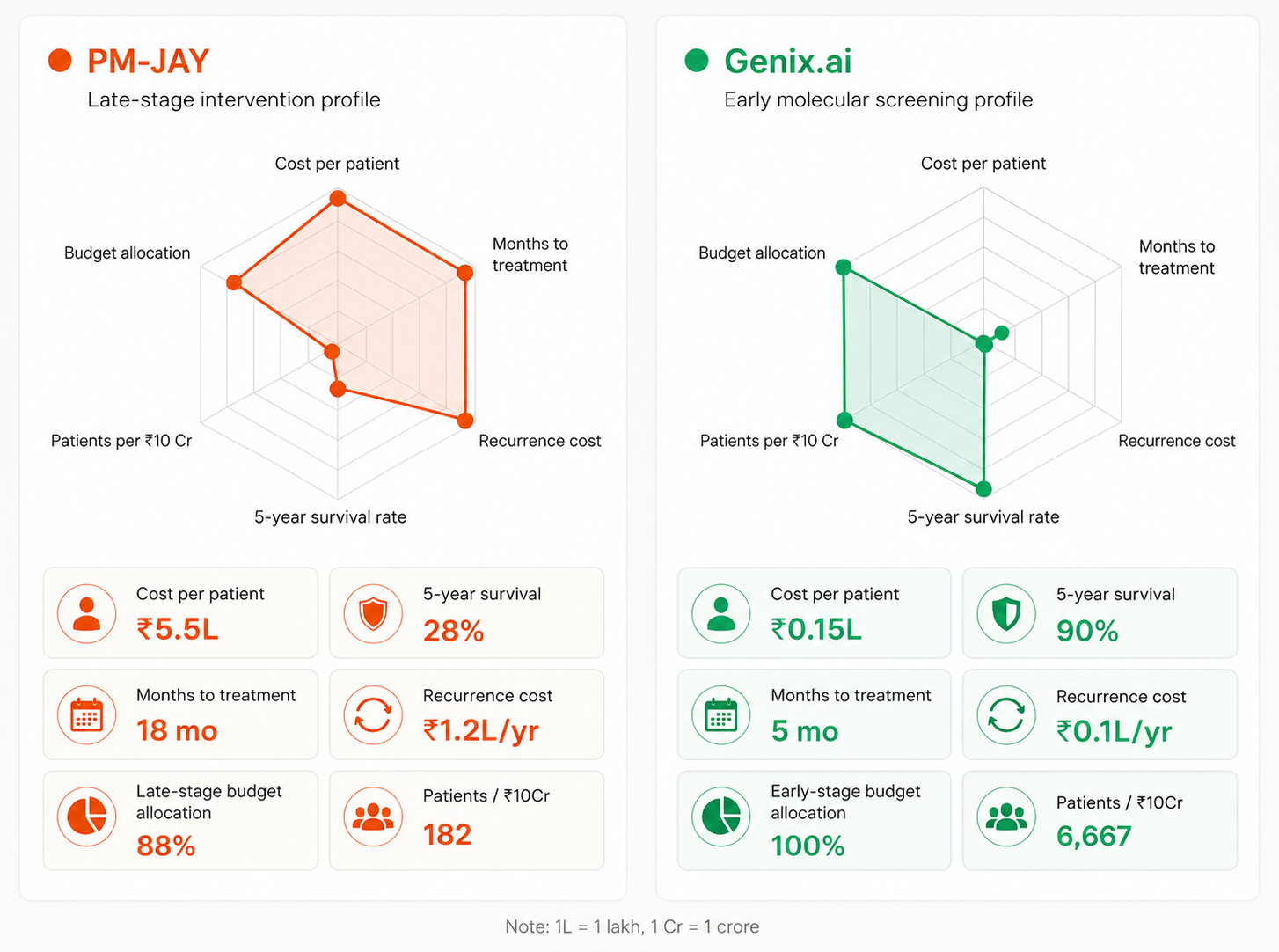
How to read them: The radar axes are normalised to 0–100. For cost, recurrence, and treatment time a larger area means worse (higher burden). For survival, patient reach, and early stage budget a larger area means better. This makes the contrast between the two charts immediately visible.
The economic divide between late stage intervention and early molecular screening is significant across every measurable metric.
Clinical Focus: Current PM-JAY claims are dominated by advanced tumor management, salvage chemotherapy regimens, and complex surgeries. Early molecular screening, by contrast, focuses on liquid biopsies, NGS based genomic risk scoring, and biomarker panels tools that identify risk before symptoms manifest.
Economic Burden: Late stage cancer care involves prolonged ICU stays, multi drug regimens, and high cost imaging all recurring over months or years. Molecular screening is a structured, one time or periodic cost with a highly predictable expenditure profile. For public health budget planners, predictability is as valuable as savings.
Patient Outcomes: Advanced stage intervention yields lower five year survival rates and high recurrence tracking costs. Early stage detection through targeted genomic profiling enables precise, personalized therapy shorter treatment durations, fewer complications, and dramatically improved survival rates. The downstream cost implications are transformative at population scale.
Scalability: AI driven diagnostic platforms can analyse NGS data, flag genomic risk variants, and generate clinical grade reports at volumes that no human specialist network can match. As India scales public health genomics, AI becomes the essential infrastructure that makes biomarker screening viable at PM-JAY's operational scale.
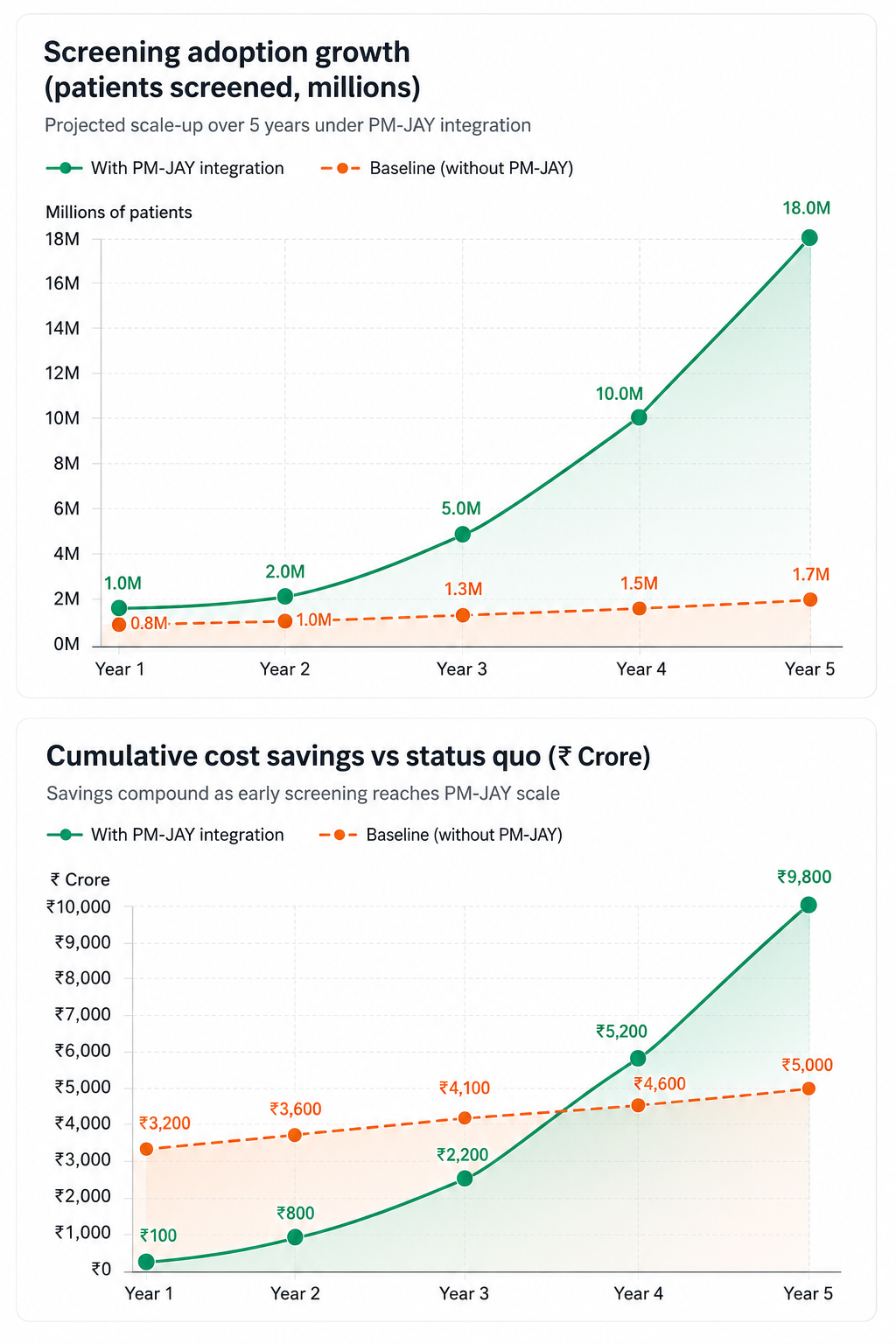
The cost saving pivot is not theoretical it follows directly from moving clinical intervention earlier on the disease curve.
The ABDM Layer: Digital Infrastructure Enabling Scalable Genomic Screening
Ayushman Bharat Digital Mission (ABDM) provides the digital backbone that makes population scale molecular screening operationally feasible. Through Health IDs, the Health Facility Registry, and interoperable health records, ABDM creates the data infrastructure needed to link genomic screening results to longitudinal patient health records.
This matters enormously for early biomarker programs. A genomic risk flag identified through an NGS panel only becomes actionable if it is connected to a patient's ongoing care pathway. ABDM's consent based health record sharing architecture means that a biomarker result generated at a diagnostic lab in Bangalore can inform a treating physician in a tier 3 town, all within a standardised, privacy compliant digital ecosystem.
For AI platforms operating in India's public health space, ABDM compliance is not optional. It is the integration standard that determines whether a precision diagnostic tool can scale beyond private urban hospitals into the public health tier the very tier where PM-JAY operates.
Why India's Cancer Burden Makes This Economically Urgent
India records approximately 1.4 million new cancer cases annually, with cervical, breast, oral, and colorectal cancers carrying the highest public health burden. The majority of these cases are diagnosed at late stages not because early detection is impossible, but because the screening infrastructure to identify them earlier does not yet exist at population scale within public health frameworks.
The economic consequence is severe. Late stage oncology care in the public system draws on high cost tertiary care budgets, strains specialist capacity, and drives families into medical poverty even under insurance protection, because many indirect and out of pocket costs are not covered.
An AI driven molecular screening program integrated into PM-JAY's preventive tier would intercept a significant proportion of these cases at Stage 0 or Stage I. The unit cost of a liquid biopsy or an NGS based panel, when standardised and procured at government scale, is a fraction of what one cycle of late stage salvage chemotherapy costs. The return on investment measured in lives extended, treatment costs avoided, and quality adjusted life years gained is one of the strongest in preventive healthcare economics.
Precision Medicine at Scale: The Technology Imperative
Scaling early biomarker detection across India's public health system requires more than political will. It requires AI native computational platforms capable of processing genomic data at population scale, with clinical grade accuracy and built in explainability for regulatory review.
Next generation sequencing pipelines must handle diverse Indian population genetics the genomic variants present in South Asian populations are distinct from those in Western reference databases, which historically dominated precision medicine research. AI platforms need to be trained on, or at minimum validated against, Indian genomic data to deliver actionable, relevant risk stratification.
Regulatory compliance across Health Insurance Portability and Accountability Act (HIPAA), General Data Protection Regulation(GDPR), Ayushman Bharat Digital Mission(ABDM), and India's emerging Digital Personal Data Protection Act(DPDP) Act must be embedded into the diagnostic workflow not bolted on as an afterthought. Public health programs operating at PM-JAY's scale require audit trails, consent management, and data sovereignty that only purpose built platforms can provide.
This is not a problem that legacy diagnostic infrastructure solves. It requires an AI native approach to genomics.
Genix.ai and the Vision for Scalable Early Detection
Genix.ai, recognised as the Best AI Platform for Genomics at THIT 2024 by Apollo Hospitals Group, is purpose built for exactly this challenge. Powered by advanced NGS, AI driven genomic interpretation, and a clinical annotation layer that translates complex variant data into actionable insights, Genix.ai operates at the intersection of health economics and precision medicine.
For India's public health system, Genix.ai's platform offers the computational infrastructure to make early biomarker screening viable at PM-JAY scale cost effective, ABDM compatible, and clinically meaningful. From oncology genomics and rare pediatric disease screening to pharmacogenomics and infectious disease profiling, Genix.ai's capabilities address the exact disease categories that currently drive the highest PM-JAY expenditure.
The mission is clear: shift personalized treatments from expensive late stage intervention to highly efficient, AI guided early stage detection and make that shift accessible across India's public health ecosystem, not only in private urban clinics.
If India's healthcare future is to be both equitable and economically sustainable, the integration of AI driven molecular screening into mass public health schemes is not a question of if. It is a question of how fast.
Explore Genix.ai's genomic intelligence platform and discover how AI-powered diagnostics can support India's transition to early, cost-effective precision medicine →genix.ai
FAQs
1. Can PM-JAY economically support early biomarker screening?
Yes early screening reduces high cost late stage treatment claims, making it a net cost reduction for public health budgets.
2. What is the difference between late stage intervention and early molecular screening economically?
Late stage care is expensive, prolonged, and unpredictable; early molecular screening is a structured, one time cost with far better clinical outcomes.
3. How does ABDM support genomic screening programs?
ABDM provides interoperable digital infrastructure Health IDs, consent based record sharing that connects genomic results to patient care pathways at scale.
4. Why do AI platforms matter for public health genomics in India?
AI platforms can process population scale NGS data with clinical accuracy, making early biomarker screening operationally feasible within public health schemes.
5. How does Genix.ai fit into India's public health genomics vision?
Genix.ai provides an ABDM compatible, AI-native platform for genomic screening and interpretation, designed to make precision diagnostics cost effective at scale.





